

Evaluation and CPR
Consists in the exploration of vital signs for the sole purpose of detecting their presence, do not stop to quantify. It should always be done quickly and systematically, by following these steps:
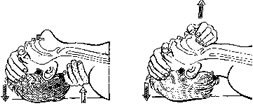
- AWARENESS: To evaluate the awareness of the victim, you should ask if he can hear you and how he is doing, while lightly shaking the shoulders or pinching his face. The expected is not only to get a verbal answer, but to react to shaking or pinching by opening or closing his eyes, or by trying to avoid our hands from his face before getting pinched, etc. (fig. 1).
- If the victim responds, we will conduct the secondary evaluation; on the other hand, the victim is unresponsive, then we should consider the victim an unconscious patient and must contact an ambulance and/or a physician before we continue to the breathing evaluation.
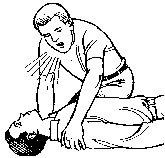
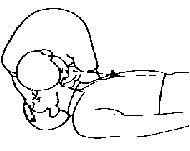
Figure 1
- PREPARATION::We will place ourselves at shoulder height, remove the clothes that may interfere with the victim’s chest (beware of the bras with metallic pieces), will loosen ties and belts, remove necklaces, chains and place the victim lying on a hard flat supine (face up) position with arms along the body.
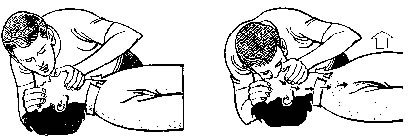
- BREATHING::We will evaluate by getting a side of our face close to the nose and mouth of the victim while we watch his chest and abdomen. By doing this, we are looking to hear and/or feel in our cheek the entry and exit of air from the victim, while allowing us to see and observe the breathing movement of the thorax and abdomen. (Fig. 2).
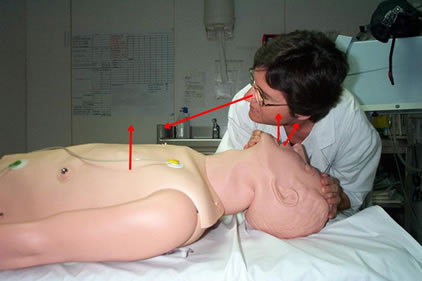
Figure 2.
In case you don’t feel the breath, observe the mouth and throat are free of objects that may obstruct the airways (dentures, gum, candy, phlegm, vomit, etc.), liberate the base of the tongue that may also block airflow through the pharynx. To do this we will put a hand on the forehead, push down, and the other in the neck, which will pull up, thereby stretching the neck and elevating the jaw bringing with it the base of the tongue, turning back to check breathing . This maneuver is known as hyperextension.
- If there is breathing, we will turn his head to one side and continue with the secondary evaluation; if on the other hand, there is no breathing, we will do 2 continuous insufflations ( mouth to mouth) and then evaluate the pulse.
- MOUTH TO MOUTH: Is to introduce into the victim’s lung the air contained in our mouth, pharynx, larynx, trachea and bronchi before it is tainted by our own breathing; that is the air that has not suffered the total gas exchange in our lungs.
- To do this, keep the victim's neck in extension, we will stick our lips tightly around the victim's mouth while pinching his nose with our index finger and thumb of the hand that remains on the forehead; we will insufflate the air with moderate strength for no more than two seconds at a time, while we look at his chest and abdomen and make sure that what goes up is the thorax.
- If while insufflating the air, what goes up is the abdomen, that is a sign that the air is passing into the stomach instead of the lungs, in this case, correct the position of the head again by doing again the hyperextension of the neck or by checking the mouth cavity and pharynx to detect the any foreign item that may prevent the entry of air into the lungs.
- PULSE: We will locate the pulse in any of the carotid arteries located in the neck on either side of the Adam’s apple. We will use 2 or 3 fingers (not thumb) of the hand we had in the neck, which we will slide down on either side of the trachea (better if it is on the opposite side to us) to the depression between it and the external muscle –cleido-mastoid, pushing towards the Adam’s apple.

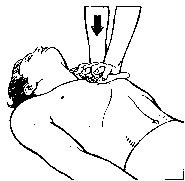
- EXTERNAL CARDIAC MASSAGE:It consists of compressing the heart between the sternum and spine loading our weight on the lower third of the sternum of the victim. To locate this point exactly, we will follow with the fingers of one of our hands the lower edge of the ribs toward the sternum, and in the central chest area we will meet the cartilaginous tip of the sternum (xiphoid process); at this point we will put 2 or 3 fingers of the other hand in the direction of the head and in this new section we’ll place the heel of the first hand. This is the area where we will do compressions to a completely naked body, especially getting metallic bras out of the way.
- To do so, without supporting your palm or fingers on the victim, we will place the other hand on top of the first one (interlacing the fingers) and with straight arms and perpendicular to the chest of the victim; we’ll drop our weight in order to lower the chest a few inches (1).
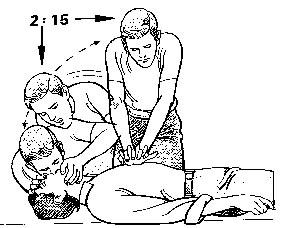
- The compressions must be fast and rhythmic (and you will be counting …. And one…and two….and three) and so on until you reach 15 compressions, then again give two quick breaths and 15 times apply external massage.
- Each set of 2 breaths and 15 massages is called a resuscitation cycle by rescuers.
- If there are two rescuers, the cycle is of 2 insufflations and 30 massages.
- A sequence consists of 4 complete cycles of resuscitation.
(1) CAUTION: Not everyone has the same consistency in his ribs, so it is recommended to quickly do one or two taps to test the hardness of the dead way and know exactly where the real pressure on the heart muscle begins.
- END OF RESUSCITATION: At the end of each sequence will return to evaluate whether the pulse is present. If there is no pulse, we will continue giving more sequences until pulse is back. When the pulse returns, we’ll evaluate breathing as described above.
We can call the resuscitation over...
- ... When someone else replace us (another rescuers, medical care personnel from an ambulance, physician, etc.)
- ... When a physician certifies the death of the victim.
- ... When the victim recovers vital signs.
- ... When we are exhausted and unable to continue with the resuscitation.
